
This summer Jerry Gurwitz, MD, longtime leader of the geriatrics division at the University of Massachusetts Medical School, had an opinion piece published in JAMA on the Paradoxical Decline of Geriatric Medicine as a Profession. I have long admired Dr. Gurwitz for his vital research on problematic prescribing, his commitment to build geriatrics within his institution, and his work to ensure that UMass physicians have the tools to deliver good care to their older patients, so I think it is worth listening when he tries to call our attention to a crisis.
And, writing from a Foundation that sees training as essential to delivering needed, equitable and high-quality coordinated care to older adults, I think he is calling our attention to a serious workforce issue that transcends medicine alone and extends to all the other health professions. There is simply a critical shortage of skilled professionals ready and able to provide expert care for our growing aging population.
For example, the entire specialization of “Geriatric Nurse Practitioner” was eliminated about 10 years ago due to low demand and replaced with “Adult and Gerontology Nurse Practitioner” which is still nowhere near as popular as “Family Nurse Practitioner.” There is no field-level specialization pathway within social work for a focus on gerontology. The specialty fields within pharmacy, occupational therapy, physical therapy, and other health professions are very small and also struggling. It just happens that the data in the field of medicine are particularly easy to access and track because the post-medical school training (known as residency) specialties of medicine are paid for by public dollars and are both formal and heavily regulated.
First the paradox Dr. Gurwitz calls out: Despite the leading edge of the baby boom hitting old-old (reaching 75 and beyond) in 2021, the number of geriatricians declined in the period 2000 to 2022 from 10,000 to 7,000. As he notes, this decline is necessarily a function of small numbers of new geriatricians entering the field and many others retiring or simply failing to recertify as geriatricians at the end of the 10-year board certification period. I actually think that the problem is both more and less serious than it might appear.
While it looks like the number of geriatricians is falling, I think it is more accurate to say that the number of people with board certification is falling. For the first several years of the existence of the specialty of geriatrics 1988-1994, there was a “practice pathway” or more realistically, an exam-only pathway to obtaining the “certificate of added qualification.” This enabled physicians who had substantial experience caring for older people to be certified without doing a fellowship. Combined with a rumor that only physicians with a Certificate of Added Qualification (CAQ) would be allowed to bill for treating Medicare beneficiaries, this led to a rush of physicians certifying by exam-only in its last few years (1988, 1990, and 1992) – almost 6,000 from internal medicine and family medicine combined. In those same years the numbers becoming board certified following a fellowship were 183, 178, and 123 in internal medicine and 43, 25, and 65 in family medicine – numbers not very different from today’s output (as shown in the chart displaying the number of first year fellows during the past 17 years). Over time, the initial bulge of physicians who certified by exam only, discovered that their certificate of qualification did nothing for them and perhaps even subjected them to adverse selection where they got the harder and lower paying patients and so let their certification lapse.
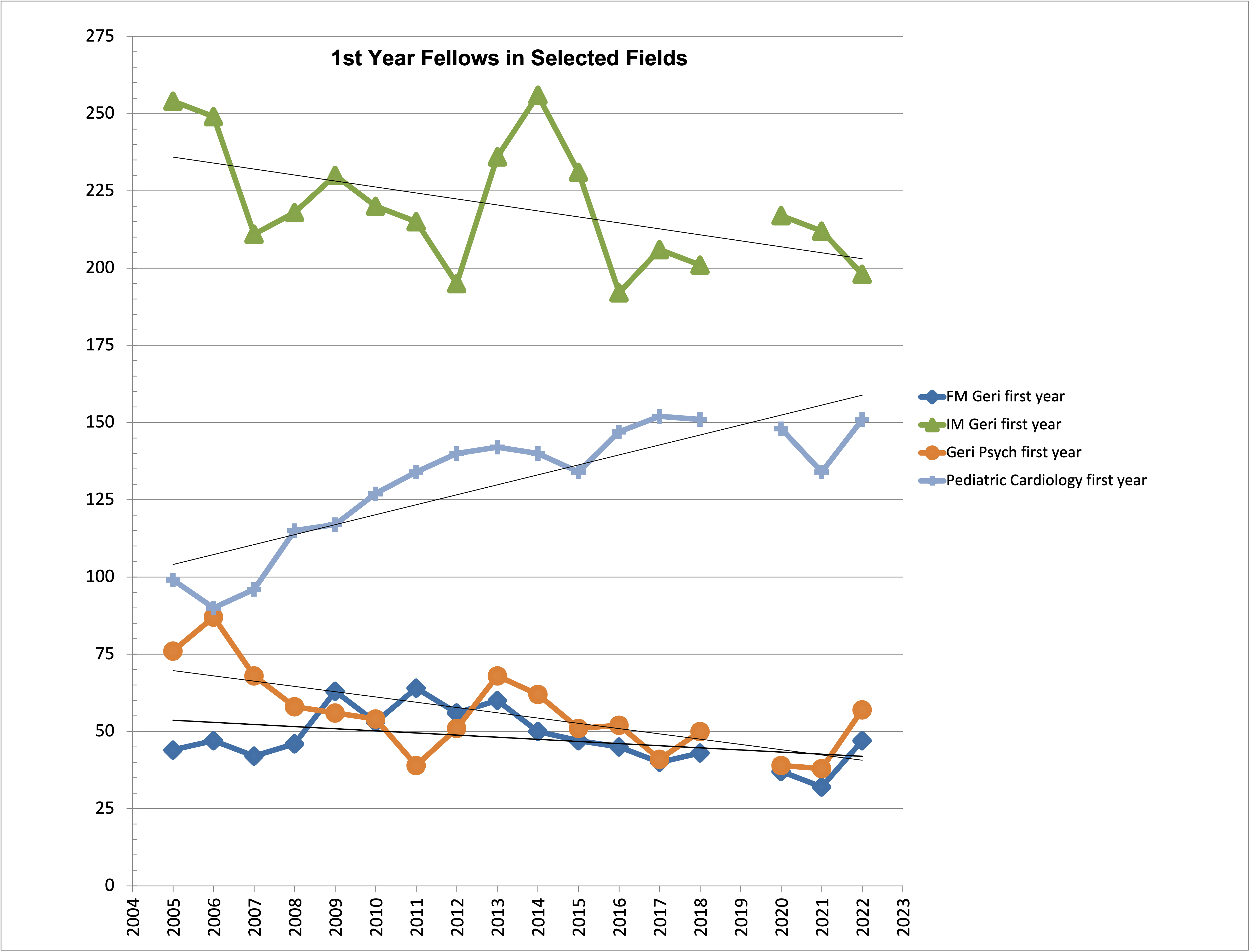
Number of geriatrics fellows in family medicine, internal medicine and psychiatry compared to number of fellows in pediatric cardiology.
What has been tried?
Reduced Fellowship Duration. Around 1998, the required duration of geriatrics fellowship was decreased from two years to one year. While this was intended to increase the attractiveness and throughput of geriatrics as a clinical practice specialty, it also made finding funding for longer periods of training for other skills (research, administration, teaching) increasingly difficult. This reduction in training time (and forgone earnings) had no effect on the number of people pursuing a geriatrics fellowship.
Subspecialty rather than Certificate of Added Qualification. Another tweak, in 2006, to training and positioning, was that for the part of geriatrics sponsored by internal medicine, geriatrics became a specialty of internal medicine rather than merely a certificate (which it remains in family medicine). This was supposed to increase prestige and reduce testing/recertification burden, but again it had no effect on the number of people entering fellowship.
Loan Forgiveness. Given the concern that primary care practitioners of all types are underpaid, which goes even more so for geriatricians, there have been multiple efforts to use financial incentives tied to the high level of educational debt that many physicians carry when they emerge into practice. Loan repayment efforts are common as incentives to research careers, rural practice setting (anyone remember the fish-out-of-water TV series “Northern Exposure” from 1990?), and in some cases geriatrics specialization. Unfortunately, these are typically small, very complicated programs that come long after future physicians have to make their choices of practice specialty. Despite the availability of such programs in California, few geriatricians get significant loan repayment, and there is no evidence that it increases the number of people specializing in the field.
Increased Pay for Practice. Oddly enough the Affordable Care Act included a 10% additional pay rate premium for practitioners billing Medicare who got the majority of their income from billing Medicare evaluation and management codes (i.e., geriatricians and other practitioners doing cognitive/non-procedural work on Medicare beneficiaries). While I’m not aware of any formal evaluation, as far as I know the experiment had no observable effect on increasing the number of geriatricians. The program has long since sunsetted, and I don’t even know how much it added to Fee-for-Service Medicare payments, much less if any of the additional money filtered through to the geriatricians earning it.
And of course, as Dr. Gurwitz points out, the growing appreciation of our national demographics has not helped either.
What can be done?
Right now, geriatrics is stuck in a downward spiral. Because there are so few, it is hard for the public to have much experience with the specialty, and thus there is no public demand. The difficulty in recruiting into the profession despite many, many ideas and initiatives has created a crisis of confidence, which then makes recruitment even harder.
So what are we going to do?
How can geriatric medicine become an attractive career, highlight its expertise, spread the principles of good care, and make itself into the growing field it should be? First, we need to recognize all the things that haven’t worked and avoid those ideas.
What could make a difference?
First, I think geriatrics needs to return its fellowship to at least two years. Especially, while the field is (re)building, it needs all the skills and credibility it can get. It needs to be sure to create business of medicine tracks as well as research tracks. We should try to ensure that geriatricians have top-flight clinical skills and really do have the knowledge to have an impact in managed care and other non-traditional/non-fee-for-service settings where macro practice can be a real thing.
Second, if you want something, you need to pay for it. Our third-party payment system (i.e., Medicare) sets prices and has virtually no mechanism for increasing price in the face of demand. Unfortunately, even if every single Medicare beneficiary knew what a geriatrician was and wanted one as much as they want an oncologist when they get cancer, it would take an act of Congress to increase payment for a particular medical specialty. And moreover, most additional payment schemes (like Medical Homes) come with additional costs for staff and practitioner time that reduce their financial benefits. They may make practice more effective and attractive, but they won’t improve the bottom line.
So, let’s take advantage of behavioral economics principles instead of trying to work against them and pay for what we want. Let’s pay residents and fellows more to study and commit to geriatrics. Many years ago, I worked up an idea of paying the debt payments of residents and geriatric fellows while in training – perhaps $18,000 to $28,000 per year at today’s interest rates for three to four years each. These payments would start exactly when people are making decisions about specialization. They would come while trainee pay was capped by graduate medical education standards (median PGY1 Resident pay is $58,000, median fellow [PGY4] pay is $72,000) and ensure that trainees could either pay down their debts or afford key parts of their lives (such as marriage and children) in their 20s or early 30s that are otherwise quite difficult to manage. Later, when making a full physician salary (> $200k even for geriatricians), making debt payments is easier, and the same-sized incentives would mean much less.
I don’t know if these efforts would solve the shortage of geriatricians, but at the very least we would be making new mistakes rather than just repeating the old ones. I believe that care of older adults is sufficiently different from caring from younger adults as to justify as much specialization in geriatrics as we see in pediatrics -- and in all the health professions, not just in medicine. We just have to have the will and discipline to make that happen.


Comments
"yes" to making the geri fellowship two years! and if these fellows were well-paid that would help too, especially as people consider what to do after fellowship.
Our seeming lack of progress can feel truly disheartening and I appreciate the perspective that it's not as bad as it looks when you take into account the historical perspective, so thank you for pointing that out.
The need is so great in both the private sector and in academic medicine; geriatricians have a lot of choice about where they'll practice and the type of practice they'll go into.
Archaic academic systems don't help matters. We need to make it easy and enjoyable for more geriatricians in private practice to teach residents and fellows. In addition, the competition for academic geriatricians is fierce so we continue to need more faculty who will teach and inspire the next generation. Understanding that medical schools have become appendages to large health systems, we must infiltrate these health systems with geriatrics.
there's a bit of a chicken-and-eggy feel to all of this. thanks to the Archstone foundation to help us and push us and challenge us!