Welcome to our first Report to the Field, intended to be an annual online publication to succeed the Biennial Reports published by Archstone Foundation for the past two decades.
While it includes the numbers you’d expect in an annual report – how much we awarded, how we allocated those grants among our strategic priorities, the share of awards to specifically support underserved communities – it’s focused on our strategic goals. As clearly as we can, we want to demonstrate to our current and prospective grantees, other philanthropies, and policymakers how we are advancing our mission to improve the health and well-being of all older Californians and their caregivers.
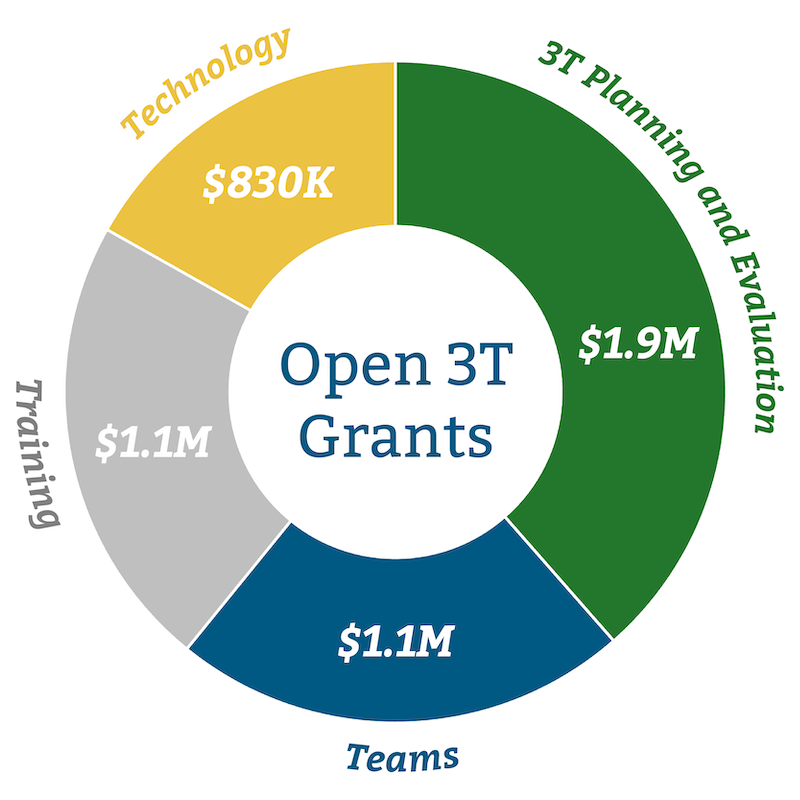
This is our first report since the Foundation began implementing its Three T’s grantmaking strategy: Teams, Training, and Technology. Promoting teams, enhancing training, and improving technology are our pillars for improving care coordination, expanding the definition of care to include social services as well as medical treatment, and ensuring that care for older Californians is increasingly equitable, just, inclusive, and embracing of diversity.
Eighteen months into our new approach, we believe we’re hitting our stride. And we’re eager to join an ever-expanding roster of partners in taking the next steps. Please read on to learn more about some of our work over the past year and our view of the future. To begin, we frame Archstone Foundation’s current thinking about our new approach by answering two essential questions.
What does equitable, coordinated care for older adults really look like?
Why is this the focus of our grantmaking?
These are the expansive questions Archstone Foundation addresses every day. We’ve learned that the answers are often found in the experiences of the people we’re serving.
Let's consider the hypothetical example of Isabella and her daughter Maria, two hard-working, low-income Californians. We are confident that if we can make the health and social support system work in a coordinated way for people like them – who have few economic reserves, limited experience with the healthcare system, and little capacity to compensate for the system’s biases and defects – we can make it work well for everyone.
Expanding a Proven, Culturally Appropriate Teamwork Model
Priority: Teams
Grantee: Public Health Institute
Amount: $510,000 over 30 months (awarded in 2021)
Project: Replicate in Los Angeles an advanced illness care program pioneered in Alameda County
Teamwork is at the core of coordinated care. And putting lay people in charge of promoting Teams (one of our Three T priorities) often yields the best results – for both team members and the people they’re caring for. That approach is being modeled by the Public Health Institute’s faith-based and person-centered AC Alliance Advanced Illness Care Program. It provides lay care navigators who help predominantly African American adults with advanced illness (and their caregivers) bridge gaps between health delivery systems, community organizations and faith-based communities.
This model of care and community engagement – focused on the medical, social, spiritual, caregiving and advanced care planning wishes of those served – is especially important in the African American community, which has a longstanding mistrust of health care systems due to past and present injustice.
With our support, AC Care Alliance is taking this program to the state’s biggest city – Los Angeles.
In Their Words
The Rev. Cynthia Carter Perrilliat Executive Director, AC Care Alliance
“Lay coordinators are crucial to providing comprehensive team care in community settings, where people feel most comfortable, because these people support patients and their families, expand the health system’s capacity, and make it more equitable for people of color.”
COORDINATED CARE: A STORY
This brief video illustrates our vision of coordinated care and how we are working to make it a reality for all older adults.
Isabella is a 75-year-old retired seamstress who resides in a rent-subsidized apartment in East Los Angeles and is living with diabetes and Parkinson’s disease. She and her late husband, who was a non-union laborer, could never get a mortgage to buy a home, and Social Security now provides almost all her income. Her principal family caregiver is her daughter, Maria, who works full-time at a local restaurant but visits several times a week. Maria has recently noticed some mental decline and depression in her mother. Isabella has lost interest in venturing out, other than for a Spanish-speaking Mass.
For Isabella and Maria, what would it mean to have equitable, high-quality coordinated care that effectively integrates health and social services – and places the person and family at the center?
Isabella’s cane slips and she falls in her apartment. A neighbor calls 911 and an ambulance takes her to a hospital where she is greeted by a Spanish-speaking triage nurse and then evaluated by a physician with an interpreter present until Maria arrives. The complexities posed by Isabella’s underlying conditions and her apparent disorientation prompt the doctor to call in a geriatrician, who convenes a team of other medical specialists, a pharmacist, and a social worker – who have recently completed training in communicating with one another as well as with older patients and caregivers. The team uses integrated technology to access Isabella’s disparate records, understand how her needs can best be served by the available benefits in Medicare and Medi-Cal, and coordinate with organizations in her community ready to provide the services she will need.
After a diagnosis is finalized and while a broken bone is being set, team members collaborate on an initial plan of comprehensive care, which they modify after talking with both Isabella and Maria – adapting the plan to address Isabella’s quality-of-life preferences and religious values, and her daughter’s work-life-balance limits and observations about conditions in her mother’s home. When Isabella is discharged, she is using a walker and a new reclining chair is on the way. Arrangements have been made for delivery of diabetic-appropriate meals, and for regular visits by a bilingual home health aide trained to use software that identifies potential interaction problems with Isabella’s new and previous medications. And Maria and Isabella have the phone number of a healthcare advocate – a promotora de salud, or community health worker.
This trained and knowledgeable community health worker helps increase Isabella’s and Maria’s health knowledge by explaining diabetes and Parkinson’s in clear and easy-to-understand language. She provides Isabella social support, team-based depression treatment and follow-up to make sure the home delivered meals are meeting her needs. She also assists Maria by providing advocacy and connecting her to community resources such as a caregiver support group.
Isabella and Maria both know they are in a phase of life where their circumstances may be changing relatively rapidly. Isabella’s conditions are not all curable, and she may soon need the additional help of a palliative care specialist, for example. But she and Maria are confident they will be at the center of shaping the next phase of care, backed by a well-trained and culturally competent team that’s bolstered by the best technology.
Preparing More Community Health Workers
Priority: Training
Grantee: Partners in Care Foundation
Amount: $480,000 over two years (awarded in 2021)
Project: Create an online care coordination course for community health workers
Community health workers provide vital coordinated care and improve health outcomes, particularly in underserved communities. But this care doesn’t happen by chance. CHWs need specific training to work in community-based organizations, physician offices, and other settings serving older adults. Preparing care providers in this way is one of the goals of the Training component of our grantmaking strategy: To address the complex care needs of older adults by training collaborative teams and translating knowledge through training programs that better equip both social service and health care practitioners.
Partners in Care Foundation used our support to develop an online training program that has now enrolled more than 300 community health workers. The San Fernando-based organization was also able to leverage the grant and expand access to the training with support from CalGrows, a state program that supports innovative ways of building the elder care workforce. Partners has already and will continue to significantly increase the number of community health workers prepared to improve the health and well-being of older Californians.
In Their Words
June Simmons President, Partners in Care Foundation
“The course better prepares CHWs to meet older adults’ needs, because now they fully understand how to provide culturally tailored resources and access supportive services including meals, transportation, and housing.”
PEOPLE AND PROVIDERS BENEFIT
This is the vision Archstone Foundation wants to realize: A California where all older adults and their caregivers, especially those with lives impacted by racial and economic inequity, can count on being the central members of care teams that adhere to patient goals and preferences when implementing holistic plans integrating high quality medical care and social services.
For both patients and providers, the benefits are clear.
Placing older people at the center of their care means they are more likely to receive not only the treatments they need and the services they want, but also none of the care they do not want. That’s one good way to define equitable care. It’s also a way to improve health outcomes as perceived by the patient. If an older woman's top priority is spending more time with her family and the care plan prioritizes that, she is more likely to understand the value of, and adhere to, whatever treatments are prescribed. So her outcome may be better for her than if she is told to follow, but then fails to follow, a strict blood sugar monitoring regimen designed to control diabetes in a quantitative way.
This approach is also good for medical and social service providers, because it reduces their frustrations with the traditional approach: Citing abstract medical reasons for taking pills or therapies, instead of explaining how those therapies will help patients achieve their goals, often doesn’t work. They don’t take their medicine, they don’t get better, they and their providers are disappointed, and health insurers have wasted money. A person-centered approach saves money and improves satisfaction for patients as well as providers, because they often get to see the professionally gratifying benefits of their healing efforts. And a comprehensive team means that an individual provider doesn’t have to problem-solve alone.
Shrinking the Digital Divide for Older Californians
Priority: Technology
Grantee: University of Southern California
Amount: $150,000 over two years (awarded in 2021)
Project: Assess a state program providing tablets to low-income older adults
The rapidly changing digital world has the power to spread the benefits of coordinated care, which is why improving Technology is one pillar of Archstone Foundation’s grantmaking strategy. But far too many older Californians, more than 1.5 million of them, are stuck on the wrong side of the digital divide – without a computing device, smartphone, or the high-speed connectivity necessary to access digital resources at home.
The state has sought to shrink this gap by providing iPads with internet connectivity, and the training to use them, to as many as 4,000 low-income or disabled older adults. The purpose of the CHAT program (for Connections, Health, Aging and Technology) was to reduce social isolation and ease access to health care, social services, and social connections during the peak in the coronavirus pandemic. But we don’t know if these devices were used or if the training was effective.
With our support, USC’s Leonard Davis School of Gerontology is assessing the program’s results, which will inform future efforts to use technology to improve the well-being of older Californians.
In Their Words
Kathleen Wilber Professor of Gerontology, USC
“Evaluating this program will help us learn how digital connectivity impacts older adults’ lives, the challenges and barriers they face in using technology, and the benefits they get from connecting.”
TOWARD A NEW PARADIGM
Getting to this point requires a systemic commitment to tearing down silos and embracing cross-discipline collaboration. It takes a wide range of additional training for providers of all kinds, especially on the particular medical and social needs of older people. And it relies on embracing the best use of technologies, especially those that can enhance the exchange of health information or improve teamwork.
In short, it requires a paradigm shift. Those are rarely quick or easy – and that is especially true when it comes to altering our healthcare system, a behemoth accounting for nearly one-fifth of the nation’s spending on goods and services every year.
Reducing disparities in outcomes is mission critical for our goal of improving health and well-being. This means an intentional and thoughtful focus throughout our grantmaking on reducing the differences among demographic groups in the rates of chronic conditions and diseases, access to health care, and mortality. Regardless of race, gender, geography, or ability, we all deserve to have access to high quality care that meets our unique needs and preferences. And we all should be able to expect similar health outcomes. This is why we’ve developed and are following our five grantmaking principles for reducing racial health disparities.
We have begun taking steps toward this ambitious goal. Our initial grants to improve Teams, Training and Technology are producing solid results and informing the next steps in our work. We’re planning those next steps with a steadily expanding network of allies – state agencies, other funders and health care providers who share our vision of a fundamentally different future. We’re also committed to tracking and sharing our progress – and changes in the field – through our partnership with RAND Corporation to create a data monitoring center and impact roadmap. This effort will provide a means to measure change in peoples’ health, track reductions in health disparities, and enable us to modify our course along the way.
Getting to the Next Level
Priority: Capacity Building and Equity
Grantee: Los Angeles LGBT Center
Amount: $50,000 (awarded in 2022)
Project: Identify services gaps and access barriers for older LGBTQ+ people of color
While the Three Ts is now the heart of our grantmaking strategy, we continue to believe in building the capacity of nonprofits seeking to improve older Californians’ health and well-being. That can include helping established organizations understand where they could be doing more.
For more than half a century the Los Angeles LGBT Center has provided accessible services and programs to support the region’s gay, lesbian, bisexual and transgender people. An estimated 65,000 are older than 65, and the center addresses the unique needs of this marginalized group. Older LGBTQ+ people of color have been particularly underserved due to their intersectional identities in multiple minority groups. And they will account for 40 percent of the region’s older LGBTQ+ population by the middle of the decade. With our support, the center is taking steps to better understand what more to do to benefit them, by conducting a study to identify gaps in services and barriers to access.
In Their Words
Kiera Pollock Director of Senior Services, LA LGBT Center
“The queer population of L.A. is quickly getting older and less white, and this needs assessment will help us understand what actions we must take to make sure we meet the needs of all the people we serve for years to come.”
Government’s Role in Shifting the Paradigm
First among our partners, is the state. The California Department of Aging and California’s Department of Health Care Services (DHCS) have a deep commitment to the Master Plan for Aging. DHCS is in the second year of a five-year timetable to implement CalAIM, which will transform Medi-Cal (the state’s name for Medicaid) in large part by including more social support services as benefits and improving coordination of care. This has created a great laboratory for testing our ideas – to make sure, for example, that the changes benefit populations we care most about, such as those with dementia and those eligible for both Medi-Cal and Medicare. It’s also an opportunity to help improve equity in care, because Medi-Cal beneficiaries are disproportionately from historically marginalized populations.
While we applaud these recent improvements in the balance of medical and social services, we know that in a time when government is challenged to meet its obligations, and medical providers feel profoundly underfunded, it will be challenging to get to the “promised land” where better social care reduces the need for medical care and can offset its early costs.
Preparing a More Diverse Group of Leaders for the Aging Field
Priority: Equity
Grantee: American Society on Aging
Amount: $150,000 over three years (awarded in 2021)
Project: Start a leadership and social justice program for people of color in the aging field
A core Archstone Foundation value is intentionally focusing on making care for older Californians more equitable, just, and inclusive. An obvious step toward that goal is creating a workforce in the field of aging that looks more like the community it serves.
With our support, the American Society on Aging – the largest multidisciplinary group in the field, with members from the business, academia, governments, and nonprofit groups who work with or for older adults – has taken on that challenge by creating ASA RISE for people of color who are early or mid-career workers in the field. It includes a 10-week course on equity and inclusive leadership skills and competencies and another 10-week session on inclusive leadership in action through allyship projects. The first 30 fellows completed the program in 2022, a second group of 32 completed their fellowships in 2023, and a third cohort will convene in 2024.
In Their Words
Patrice L. Dickerson Director of Programs and Thought Leadership, ASA
“Our first ASA RISE alumni are already rising up. They are stepping assuredly into leadership roles, taking seats at decision-making tables, and bringing an equity-centric lens to conversations on inclusion and belonging in their local communities, their states, and nationwide.”
Learning from Our Past to Guide Our Future
Priority: Sustaining our legacy work
Grantee: University of Washington and University of California at Davis
Amount: $3.3 million over 7 years (awarded in 2017)
Project: Support the final phase of the Care Partners Depression in Late-Life Initiative
An important piece of our previous grantmaking portfolio, this project has also provided inspiration for our new focus on integrated care.
Care Partners developed innovative approaches to treating depression late in life, in partnership with family members and community-based organizations. Built upon a highly effective collaborative care model – which utilizes teams including primary care providers, behavioral health care managers, and psychiatric consultants – it extended the reach of the team beyond the clinic walls to effectively reduce depression among racially and ethnically diverse older adults. This innovative approach also showed that confronting the social drivers of health is not only possible but also an effective way for primary care clinics to treat late-life depression.
One more success of this initiative is that it demonstrated how high-quality care should put patients at the center and be provided by a well-trained team supported by the best technology. In other words, Care Partners helped lay the cornerstones of our Three Ts strategy.
In Their Words
Jürgen Unützer Professor, University of Washington (and an Archstone Foundation board member)
“Care Partners showed how sharing and coordinating care across disciplines and agencies is challenging. It also showed that training is essential for building and sustaining teams that can surmount those challenges, and how technology can facilitate those collaborations. When these three forces come together effectively, we have something powerful.”
THE YEAR AHEAD
Our aging-focused philanthropic community has been taking small steps for decades – demonstrating effective models of team care, the benefits of training, and the need for technological improvements. Our collective effort has developed conceptual support and solid evidence. Putting all of the findings into action – all at once and at scale – is the current, ultimate challenge.
We are proud of our grants and grantees, but we know those projects by themselves will not directly translate into the broad systems change we need. They will create focal examples of the transformation we seek in the systems around a population (e.g., families living with dementia) or a locality (e.g., access to palliative care options in South Central Los Angeles). We will then need to use these successes to persuade governments, health systems, and the public to make the changes in payment, regulation, and expectations that are needed to take our vision to full scale. We know it will be hard but we are truly committed to improving the health and well-being of older Californians and their caregivers.